|
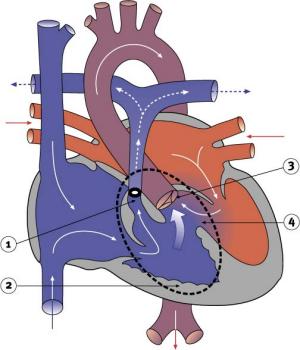
Tetralogy of FallotTetralogy of Fallot involves four defects within the heart. The first is a hole in the ventricular septum or a VSD. Second, the aorta, which is normally attached to the left ventricle, is wrongly positioned overtop the ventricular septum (and is termed an overriding aorta). Third, there is thickening (in medical terms, hypertrophy) of the muscle of the right ventricle (referred to as right ventricular hypertrophy). The fourth condition is a partial or complete obstruction of blood flow from the right ventricle (also termed RVOT-right ventricular outflow tract obstruction). This most often results from pulmonary narrowing (or, in medical terms, stenosis). Pulmonary stenosis is a narrowing of the vessels carrying blood from the right ventricle to the lungs. This narrowing is caused by an underdevelopment of the area around the lung valve and along the pulmonary arteries, and can range from a blockage at the valve to thickening below the valve. There can also be narrowing of the pulmonary artery above the valve, and the vessel can narrow into both of the branches that go to the lungs.
To provide relief for the lack of blood flow created by the pulmonary stenosis, it is usually necessary to insert a small tube as an artificial shunt. This shunt then connects the aorta (or one of its branches, such as the subclavian artery) to one of the pulmonary arteries. The best size for the shunt will depend on the size of the patient, as well as the specific structure of the patient's heart and blood vessels. Such shunts are often referred to as Blalock-Taussig shunts, after the surgeons who developed them, and are used in a variety of pediatric cardiac procedures. Depending on the artery to which the shunt is connected, they are known as either classic or modified Blalock-Taussig shunts. Children with Tetralogy of Fallot are often referred to as Tet babies. Some children with this condition also suffer from weight loss or fail to gain weight (known medically as failure to thrive). Other Tet babies suffer Tet spells or periods when they are extremely cyanotic. Symptoms include anxiety, air hunger, respiratory distress, increasing cyanosis and an altered level of consciousness. The symptoms are most often brought on by activity. Tet spells usually indicate an urgent need for repair of the heart defect. The operation to correct Tetralogy of Fallot consists of removing the outflow tract obstruction and patching the VSD. Care must be taken not to damage the heart's electrical conduction system because of the nature of the operation. Damage to the heart's electrical conduction system can interfere with the heart's ability to beat properly. Most often, complete correction of the lesions is performed, even in newborns. Palliative procedures are reserved for those patients with extremely abnormal hearts, such as those with severe underdevelopment (hypoplasia) of the pulmonary arteries and certain abnormalities of the coronary arteries. (A palliative procedure is one that alleviates the current problem but is not a definitive repair and does not usually offer a long-term good outcome.)
|
| Current | Home - Table of Contents - Chapter 2 - Tetralogy of Fallot |
| Next | Atrioventricular canal defect |
| Previous | Septal defects |
| Section 1 | Chapter 1 - Introduction to the Issues |
| Chapter 2 - Pediatric Cardiac Issues | |
| Chapter 3 - The Diagnosis of Pediatric Heart Defects and their Surgical Treatment | |
| Chapter 4 - The Health Sciences Centre | |
| Section 2 | Chapter 5 - Pediatric Cardiac Surgery in Winnipeg 1950-1993 |
| Chapter 6 - The Restart of Pediatric Cardiac Surgery in 1994 January 1, 1994 to May 17, 1994 |
|
| Chapter 7 - The Slowdown May 17 to September 1994 |
|
| Chapter 8 - Events Leading to the Suspension of the Program September 7, 1994 to December 23, 1994 |
|
| Chapter 9 - 1995 - The Aftermath of the Shutdown January to March, 1995 |
|
| Section 3 | Chapter 10 - Findings and Recommendations |
| Appendix 1 - Glossary of terms used in this report | |
| Appendix 2 - Parties to the Proceedings and counsel | |
| Appendix 3 - List of witnesses and dates of testimony | |
| Diagrams | |
| Tables | |