|
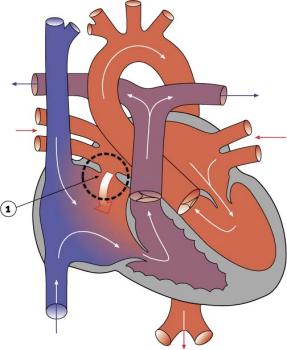
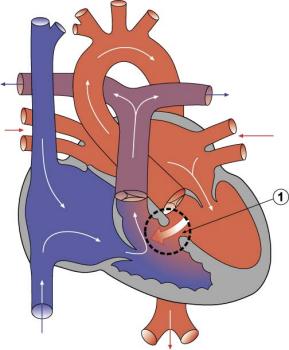
Septal defectsThe most common pediatric cardiac problems result from defects in the wall separating the right and left sides of the heart. The wall is called the septum, while the defects are referred to as septal defects. The wall between the atria is called the atrial septum and the wall between the ventricles is called the ventricular septum. A defect in the wall between the atria is referred to as an ASD, or atrial septal defect, and a defect in the wall between the ventricles is called a VSD, or ventricular septal defect. The defect can range from a small hole in the septum to a significant portion of the septum actually being missing. When there is such a defect, shunting can occur. If blood flows from the right side of the heart to the left, the child may appear blue because of the lack of oxygen in the blood. The medical term for this reduced oxygen supply is cyanosis, and a baby with blue colouring is described as being cyanotic. With some septal defects, blood may actually flow back and forth between the right and left sides of the heart. Some VSDs occur at a higher point on the septal wall, where the septum is thinner. These are referred to as perimembranous VSDs. Those VSDs that occur at a lower point on the septal wall, where the septum is thicker, are called muscular VSDs, which may be single or multiple. Other VSDs occur just below the aortic valve and are referred to as subaortic VSDs.
Some ASDs and VSDs can heal or close on their own, but in a significant number of patients, surgery is required to repair them. Repairs can take the form of a suture (or stitch) being used to close the opening if it is small enough, or a patch actually being sewn over the opening in the case of larger defects. Such patches are usually made of the patient's own pericardium or inert material such as teflon. Pericardial tissue is preferred, since it stands a smaller chance of infection or rejection and can usually grow along with the heart itself.
|
| Current | Home - Table of Contents - Chapter 2 - Septal defects |
| Next | Tetralogy of Fallot |
| Previous | Patent ductus arteriosus (PDA) |
| Section 1 | Chapter 1 - Introduction to the Issues |
| Chapter 2 - Pediatric Cardiac Issues | |
| Chapter 3 - The Diagnosis of Pediatric Heart Defects and their Surgical Treatment | |
| Chapter 4 - The Health Sciences Centre | |
| Section 2 | Chapter 5 - Pediatric Cardiac Surgery in Winnipeg 1950-1993 |
| Chapter 6 - The Restart of Pediatric Cardiac Surgery in 1994 January 1, 1994 to May 17, 1994 |
|
| Chapter 7 - The Slowdown May 17 to September 1994 |
|
| Chapter 8 - Events Leading to the Suspension of the Program September 7, 1994 to December 23, 1994 |
|
| Chapter 9 - 1995 - The Aftermath of the Shutdown January to March, 1995 |
|
| Section 3 | Chapter 10 - Findings and Recommendations |
| Appendix 1 - Glossary of terms used in this report | |
| Appendix 2 - Parties to the Proceedings and counsel | |
| Appendix 3 - List of witnesses and dates of testimony | |
| Diagrams | |
| Tables | |