|
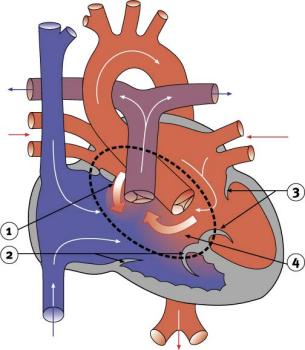
Atrioventricular canal defectAtrioventricular (AV) canal defect is a large hole in the centre of the heart. The defect is situated where the septal wall between the upper chambers (atria) joins the septal wall between the lower chambers (ventricles). In addition, the tricuspid and mitral valves (the atrioventricular valves), which normally separate the heart's upper and lower chambers, are not formed as individual valves. Instead, one large valve bridges the defect.
Complete AV canal defect, also known as an atrioventricular septal defect or endocardial cushion defect, is often associated with other cardiac defects, such as Tetralogy of Fallot. The complete AV canal defect is commonly found in children with Down's syndrome. An incomplete or partial form of AV canal defect, known as an ostium primum atrial septal defect, involves only the atrial septum. The AV canal defect lets some of the oxygen-rich blood from the heart's left side pass (or shunt) back into the heart's right side. There, the oxygen-rich blood mixes with the oxygen-poor venous blood from the body and is sent back to the lungs. This results in the heart pumping an extra amount of blood and working harder than it should. In time, the extra work causes the heart to enlarge. There is also an associated increase in the pressure in the pulmonary artery, which may cause problems. With complete AV canal defects, signs and symptoms occur early in infancy. These usually include abnormal heart sounds, congestive heart failure, intermittent cyanosis, respiratory infections, poor feeding and inadequate weight gain. In a baby with severe symptoms or high pulmonary artery pressure, surgery must usually be done in infancy. The surgeon closes the hole with one or two patches. The single valve is then divided between the atria and the ventricles to make two separate valves. Again, care must be taken not to damage the heart's electrical conduction system.
|
| Current | Home - Table of Contents - Chapter 2 - Atrioventricular canal defect |
| Next | Coarctation of the aorta |
| Previous | Tetralogy of Fallot |
| Section 1 | Chapter 1 - Introduction to the Issues |
| Chapter 2 - Pediatric Cardiac Issues | |
| Chapter 3 - The Diagnosis of Pediatric Heart Defects and their Surgical Treatment | |
| Chapter 4 - The Health Sciences Centre | |
| Section 2 | Chapter 5 - Pediatric Cardiac Surgery in Winnipeg 1950-1993 |
| Chapter 6 - The Restart of Pediatric Cardiac Surgery in 1994 January 1, 1994 to May 17, 1994 |
|
| Chapter 7 - The Slowdown May 17 to September 1994 |
|
| Chapter 8 - Events Leading to the Suspension of the Program September 7, 1994 to December 23, 1994 |
|
| Chapter 9 - 1995 - The Aftermath of the Shutdown January to March, 1995 |
|
| Section 3 | Chapter 10 - Findings and Recommendations |
| Appendix 1 - Glossary of terms used in this report | |
| Appendix 2 - Parties to the Proceedings and counsel | |
| Appendix 3 - List of witnesses and dates of testimony | |
| Diagrams | |
| Tables | |