|
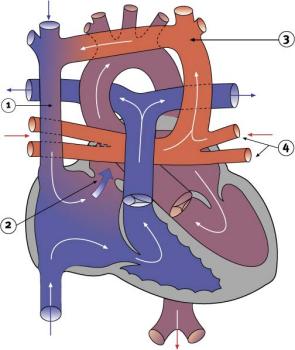
Total anomalous pulmonary venous connectionThe pulmonary veins usually connect to the left atrium. However, in total anomalous pulmonary venous connection (TAPVC), there is no direct connection between any pulmonary vein and the left atrium. The pulmonary veins that normally bring oxygen-rich blood back from the lung are not connected to the left atrium. Instead, they drain through abnormal connections to the right atrium. In the right atrium, the oxygen-rich blood from the pulmonary veins mixes with the oxygen-poor venous blood from the body. Some of this mixture then passes through an atrial septal defect or a PFO into the left atrium. The result is that the blood flowing to the body is poorly oxygenated. The rest of the poorly oxygenated mixture flows through the right ventricle into the pulmonary artery and on to the lungs. Both congestive heart failure and pulmonary artery hypertension may develop. Signs of these may appear soon after birth and vary in severity. They include a lethargic appearance, pallor or cyanosis, poor feeding and weight loss. TAPVC is usually repaired in early infancy or when the abnormality is diagnosed. Surgical repair involves reconnecting the pulmonary veins to the left atrium and closing the atrial septal defect or PFO.
|
| Current | Home - Table of Contents - Chapter 2 - Total anomalous pulmonary venous connection |
| Next | Partial anomalous pulmonary venous drainage |
| Previous | Pulmonary atresia |
| Section 1 | Chapter 1 - Introduction to the Issues |
| Chapter 2 - Pediatric Cardiac Issues | |
| Chapter 3 - The Diagnosis of Pediatric Heart Defects and their Surgical Treatment | |
| Chapter 4 - The Health Sciences Centre | |
| Section 2 | Chapter 5 - Pediatric Cardiac Surgery in Winnipeg 1950-1993 |
| Chapter 6 - The Restart of Pediatric Cardiac Surgery in 1994 January 1, 1994 to May 17, 1994 |
|
| Chapter 7 - The Slowdown May 17 to September 1994 |
|
| Chapter 8 - Events Leading to the Suspension of the Program September 7, 1994 to December 23, 1994 |
|
| Chapter 9 - 1995 - The Aftermath of the Shutdown January to March, 1995 |
|
| Section 3 | Chapter 10 - Findings and Recommendations |
| Appendix 1 - Glossary of terms used in this report | |
| Appendix 2 - Parties to the Proceedings and counsel | |
| Appendix 3 - List of witnesses and dates of testimony | |
| Diagrams | |
| Tables | |