|
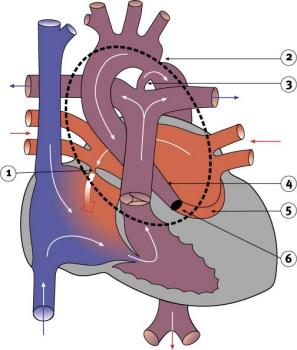
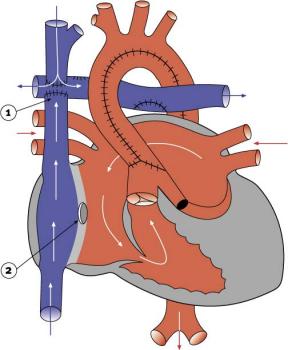
Hypoplastic left heart syndromeHypoplastic left heart syndrome (HLHS) refers to the grouping of certain congenital cardiac defects. The main characteristics are the marked hypoplasia (underdevelopment) or even absence of the left ventricle and severe hypoplasia of the aorta. Often a localized pinching (coarctation) of the aorta is also present. The main pulmonary artery is enlarged, and gives rise to a large ductus arteriosus. This allows blood to flow from the right ventricle into the aorta and out to the body. Other characteristics of HLHS often include a combination of aortic and mitral stenosis or aortic and mitral atresia.
HLHS is also used to describe cases in which the right ventricle is hypoplastic and the child also suffers from transposition of the great arteries. In such cases the hypoplastic right heart pumps into the same artery that the left ventricle normally pumps blood through, and therefore the circulation is the same as in HLHS. This is sometimes referred to as functional HLHS.
HLHS is a severe form of congenital heart disease. Without surgical intervention, HLHS is fatal. Infants are often diagnosed within 24 to 48 hours of birth. Symptoms appear when the ductus arteriosus begins to close. There are three options for treating these children: supportive care until death occurs, staged reconstruction of the heart, or a heart transplant.
Before surgical treatment was developed, at least 90 per cent of infants with this condition died by the age of one month. Even today, some infants are not candidates for surgical therapy. For these infants, supportive care is the only option. Exactly what this care entails will depend on the condition of the infant, but would likely include assistance with breathing, the provision of fluids and management of pain.
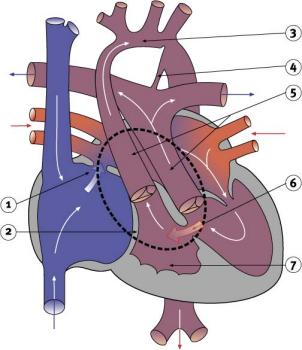
Staged reconstruction is the treatment of choice for hypoplastic left heart syndrome. Reconstruction takes place in three stages. The first stage, known as a Norwood operation, is undertaken as soon as possible after birth. This stage calls for a homograft1 to be used to enlarge the rudimentary aortic arch and then join it to the pulmonary trunk. This is known as an anastomosis. The pulmonary trunk will have been disconnected from the left and right pulmonary arteries. The newly created blood vessel functions as the patient's aorta. The right ventricle then becomes a common ventricle, pumping blood through the aorta to the rest of the body. Blood flow to the lungs is provided by means of a modified Blalock-Taussig shunt joining the innominate artery to the pulmonary artery. This increases the flow of oxygen-enriched blood that will be sent to the body. The Norwood operation also involves making a hole in the wall between the left and right atria. In medical terms this is known as an atrial septectomy.
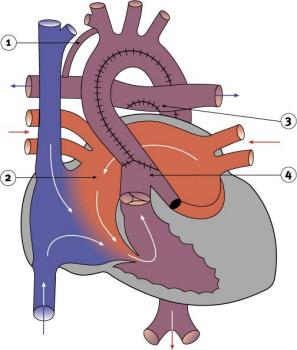
After the Norwood operation, children require medical management with various drugs. Some drugs, such as digoxin, are needed to improve the strength of the heart's contractions, and other drugs, such as diuretics, are required to remove excess fluid from the body. The second stage of reconstruction is undertaken between three and ten months of age. Stage two involves performing a bidirectional Glenn shunt or a hemi-Fontan. (This is also known as a partial Fontan or a Bidirectional Cavo-Pulmonary Shunt.) A bidirectional Glenn shunt is performed by connecting the superior vena cava (SVC) to the right branch of the pulmonary artery. As a result, venous blood from the head and upper limbs will pass directly to the lungs, bypassing the right ventricle. However, the venous blood from the lower half of the body will continue to return to the heart. While avoiding the risk of failure of a complete Fontan operation, the partial Fontan helps to relieve symptoms. The procedure decreases the volume of blood delivered to the single ventricle, thus reducing the amount of work that the ventricle must perform. Post-operatively, oxygen saturation is improved. In addition, because the bi-directional Glenn is a low-pressure shunt, it does not carry the risk of causing thickening and hardening of the blood vessels of the lungs. (This is a normal response of the lung's blood vessels to high pressures.) This operation creates a more favorable setting in which to complete a Fontan reconstruction at one and a half to two years of age.
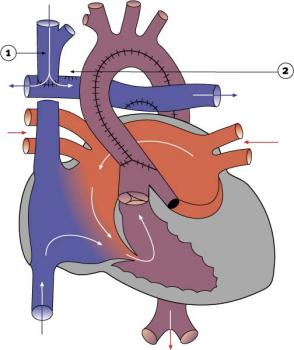
At 18 to 24 months of age, if the patient does well after the Glenn shunt and pulmonary resistance remains low, the third stage of reconstruction is possible. This involves the completion of the Fontan procedure (as described in the earlier discussion of tricuspid atresia). With the Fontan operation, the venous blood from the lower part of the body is also diverted to the lungs, thus creating the 'complete' Fontan circulation. However, if the child is not well or the pulmonary resistance is considered too high, then no further surgical treatment is possible.
Heart transplantation is carried out using the same basic techniques as for other transplants. In the case of pediatric heart transplants, the greatest problem is that infant donor hearts are in short supply. Thus transplantation is a treatment for only a limited number of babies with hypoplastic left heart syndrome. In addition, recipients can survive only with the assistance of heavy doses of expensive medication to prevent rejection of the transplanted tissue. These drugs also have significant side-effects, such as the risk of infection and lymphatic cancer, and must be taken by recipients for the rest of their lives. For those reasons, heart transplants are not considered the standard treatment for children suffering from HLHS.
|
| Current | Home - Table of Contents - Chapter 2 - Hypoplastic left heart syndrome |
| Next | Summary |
| Previous | Double outlet right ventricle |
| Section 1 | Chapter 1 - Introduction to the Issues |
| Chapter 2 - Pediatric Cardiac Issues | |
| Chapter 3 - The Diagnosis of Pediatric Heart Defects and their Surgical Treatment | |
| Chapter 4 - The Health Sciences Centre | |
| Section 2 | Chapter 5 - Pediatric Cardiac Surgery in Winnipeg 1950-1993 |
| Chapter 6 - The Restart of Pediatric Cardiac Surgery in 1994 January 1, 1994 to May 17, 1994 |
|
| Chapter 7 - The Slowdown May 17 to September 1994 |
|
| Chapter 8 - Events Leading to the Suspension of the Program September 7, 1994 to December 23, 1994 |
|
| Chapter 9 - 1995 - The Aftermath of the Shutdown January to March, 1995 |
|
| Section 3 | Chapter 10 - Findings and Recommendations |
| Appendix 1 - Glossary of terms used in this report | |
| Appendix 2 - Parties to the Proceedings and counsel | |
| Appendix 3 - List of witnesses and dates of testimony | |
| Diagrams | |
| Tables | |